An unexpected period of living rough while on his OE, gave Grant Brookes a taste of “how the other half lives” and deepened his drive to advocate for human rights. As part of a series on the NZNO board directors, Brookes spoke to Kaitiaki about his story.
Caring for his Scottish grandmother in her final months was a turning point for Grant Brookes and opened his mind to a nursing career.
“My grandmother, who I was very close to, became very sick and over the course of six to 12 months it became clear she wasn’t going to survive and the family cared for her, and I was part of that roster,” he said.
During this period, Brookes, now 54, decided to volunteer at a local hospice to get a closer look at nursing, before deciding the profession was his calling.
Grant Brookes received a scholarship to private boys school
In 1992, and in his mid-20s, Brookes began a bachelor of nursing at Otago Polytechnic – one of the first degree programmes to be offered in New Zealand.
He had spent six years as a university student, completing an honors degree in physics, before turning to the arts, studying comparative literature, philosophy and religion.
Scottish reformer heritage shows through
Brookes says his passion for education and activism connects him with his ancestors, who, as part of a breakaway protestant movement, left Scotland for the colonies, to establish new communities founded on democracy, education and egalitarianism.
The Brookes clan arrived in Dunedin on the Cornwall in 1849.
“I can see how these historical forces have shaped who I am.”
Fast forward to the late 1960s, and 1970s, Brookes describes a happy, middle-class upbringing in which academic achievement was highly valued – and quite a bit of tennis.
Grant Brookes got involved in the student protest movement in the late 1980s.
His mother pursued tertiary education in adulthood, eventually completing a doctorate in philosophy and becoming an academic.
Brookes’ father spent summers working full-time as a professional tennis coach. “His claim to fame was being the tennis coach for the New Zealand Davis Cup team,” Brookes said.
But in 1980, things changed dramatically when his father died suddenly. Brookes was just 12-years-old.
A teenaged Brookes gained a scholarship to attend John McGlashan College, a private boys high school where he thrived on academic success, debate and public speaking.
At university, Brookes got involved with the student protest movement, which ramped up in the late 1980s, in opposition to the introduction of student fees.
Academic to nurse
As a student nurse at Otago Polytechnic, Brookes admits his academic experience and love of debate didn’t go down very well.
“I was debating all sorts of moot points and they were saying: just get on and bloody well do it. In the end we met somewhere in the middle.”
During his nursing degree, Brookes came into contact with, and embraced, the Treaty of Waitangi “in a serious way” for the first time, he says.
“Growing up in Dunedin, going to a private school, I think I can only remember one Māori student in my school in the time I was there – it wasn’t in my world until I went nursing.”
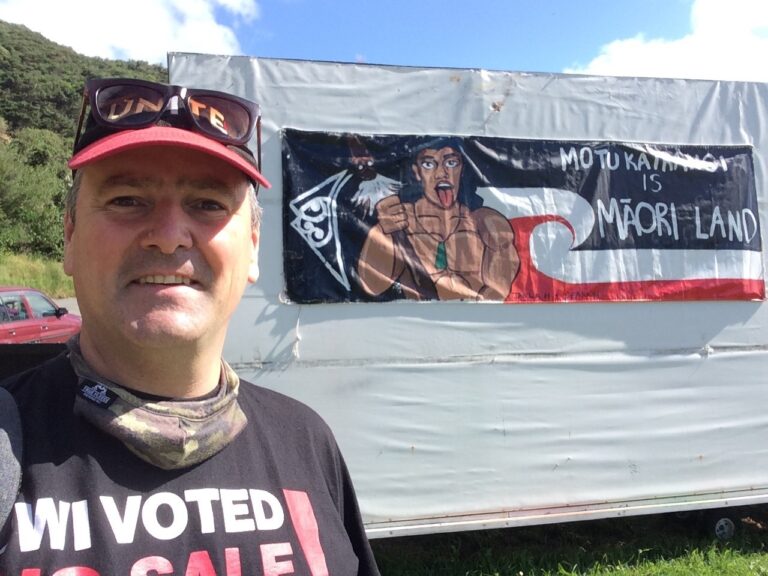
Grant Brookes at a protest in support of returning land to Māori ownership.
Grant Brookes said he became aware of te Tiriti “in a serious way” during his nursing studies.
A gap year in London which didn’t go as planned resulted in him living rough for several months, Brookes says.
After being robbed, he was declined a social welfare grant as he didn’t have British citizenship. Unable to pay rent, he lived on the streets.
“I experienced what life is like for migrants who don’t have the right residency or citizenship.”
Eventually he “clawed his way back” and got a job in a cafe, where accommodation was provided.
In New Zealand, Brookes faced a barren employment landscape after graduating in 1996.
“This was a time of dramatic health spending cuts, privatisation of health services, staff retrenchments, de-unionisation.”
From textbooks to nursing life
Brookes had decided to specialise in mental health nursing as there were “mental health issues in my family background”, but with no jobs available in Dunedin, he moved to Auckland.
During a new graduate programme, he gained experience in the different areas of mental health and came to terms with a system he felt was overly controlling of patients’ behaviour.
Despite his misgivings, Brookes said he was inspired to stay in the sector and work for improvements and “make it more respectful of human rights”.
For the past 20 years, Brookes has worked at Te Whare O Matairangi, an adult acute inpatient unit in Wellington as an employee of the former Capital and Coast DHB – now Te Whatu Ora.
NZNO board member Grant Brookes became a delegate while working as a mental health nurse in Wellington in the early 2000s.
While in this role, Brookes joined Tōpūtanga Tapuhi Kaitiaki o Aotearoa, New Zealand Nurses Organisation (NZNO), and became a delegate.
During his first year on the ward, there were three serious adverse events, which sparked numerous investigations and, eventually improvements, he said.
“There used to be three acute adult inpatient wards for the greater Wellington region and the powers-that-be decided to shut one of them, and we went down to two. The pressure on our ward went through the roof and we were not able to cope.”
He said the ward is safer than when he started, but the issue of violence – against patients and staff – had not been “solved”.
Brookes said he was fortunate to have avoided serious injuries from assaults. In his early days on the ward, a patient knocked him out with a punch.
NZNO board member Grant Brookes with his wife Linda and children Tama and Rosa-Marama in 2012.
“I found myself flat on my back on the concrete and I came to and I thought that wasn’t supposed to happen.”
But he says this was the only serious assault he has suffered in the role, ” . . . that’s pretty good going as far as the averages go”.
Over the past two years staffing levels had decreased and the ward was often short-staffed, he said.
“Things got really bad after I started [working on the ward], because many people left, and then we built that back up – but things have deteriorated. We’re not back where we started, but it’s the worst it’s been in quite a few years.”
Time for activism
Having a stable job had allowed Brookes to focus on activism for various causes, including worker rights, the landbank movement for Māori, justice for migrants and refugees, climate justice, and peace, he says.
Grant Brookes was elected on to the NZNO board this year.
This year Brookes has taken on a role as national coordinator for a group of health professionals advocating for climate change action, Ora Taiao – the NZ climate and health council, and is motivated to see the NZNO board achieve more in this area.
His recent election to the board as a director will be Brookes’ second experience in NZNO governance, following a period as president from 2018-2020.
He believes NZNO was in a “painful transition” period during that time ” . . . from being a fairly conservative professional association which did collective bargaining, into a progressive, member-driven, industrial union for professional nurses.”
The experience on the current board, which met for the first time since the elections in October, was very different to his previous experience, Brookes said.
He was certain NZNO leadership and governance would work together to achieve the aims of Maranga Mai!
* First published by kaitiaki.org.nz. Re-posted with permission.
The results of the NZNO election have been released by the Returning Officer. Lizzy, Grant and Saju would like to thank everyone who participated. We have appreciated all the kōrero people have shared with us during the election campaign, which enabled us to gain greater insights into the issues we all face. We are especially grateful for the amazing support we received from our fellow NZNO members, which meant that Grant and Saju emerge as the two top-polling candidates.
Although we are very disappointed that Lizzy missed out on being elected by just 17 votes, Grant and Saju will now work collaboratively with others to implement the policies all three of us campaigned on:
• Our member-driven union achieving safe staffing & fair pay for ALL members in ALL sectors • Our union governed with genuine bicultural partnerships • Our union being for everyone, including greater support for IQNs with a Migrant Nurses Section
At 6.31%, the voter turnout was almost exactly the same as the 2020 Board by-election (6.32%) and down slightly from the triennial Board elections in 2019 (8.11%) and 2016 (8.17%). Clearly the pattern of very low voter participation continues, which suggests to us that the visibility of the Board and understanding of its role are also very low among the NZNO membership.
Lizzy, Grant and Saju will continue to work together as and look forward to further strengthening our connections with union members. People are welcome to contact us at any time through this, our shared Facebook page.
Our Section is particularly affected by the MoU signed between NZNO and PSA which requires that mental health nurses in Waitematā, Auckland, Counties Manukau, Marlborough/Nelson and West Coast DHB areas join the PSA for industrial coverage. Those members have no choice of their primary bargaining authority. We are concerned that our members who have no choice in their selection of the PSA may be precluded from engaging in committee membership. This would reduce the pool of members who might wish to be involved in section participation such as holding office.
Thank you for your consideration of this matter.
Helen Garrick
Chair, MHNS Committee
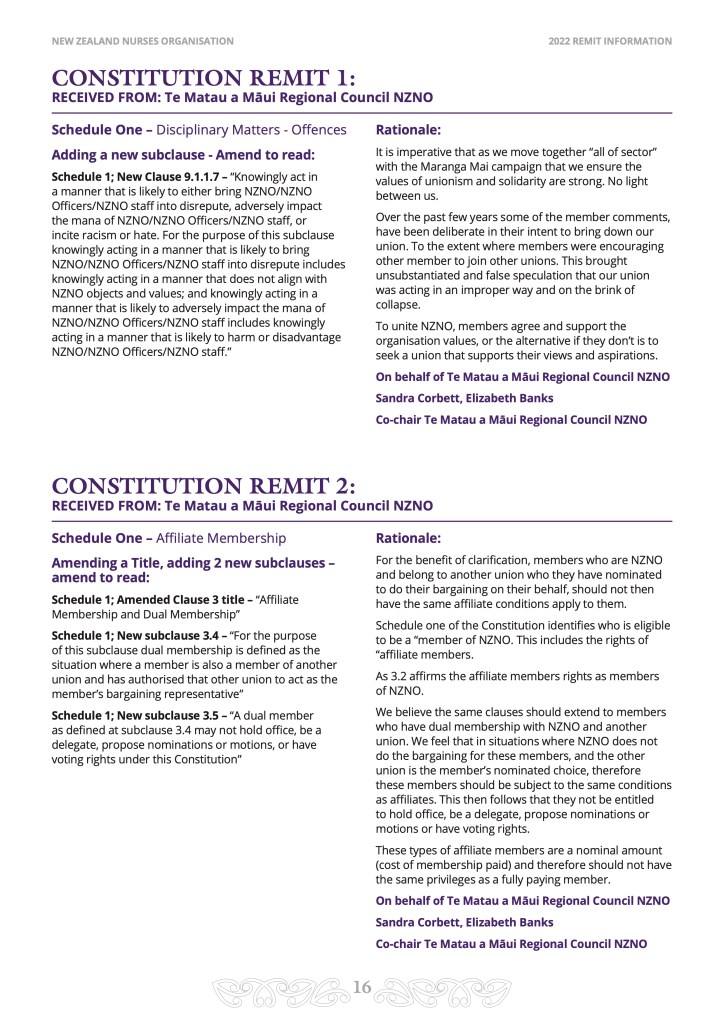
• Re-posted with permission. A personal message from the MHNS Secretary is also available here. Text of the Remit is below.
Crystal balls are not part of the evidenced-based toolkit of a Mental Health Nurse. If they were, we might know for certain what the future holds for us in this time of system change. As things stand, however, past events are a fair predictor of what we can expect.
Last month’s much-anticipated “Wellbeing Budget” sadly failed to live up to its name. As NZNO Chief Executive Paul Goulter explained, “We’re looking forward to getting some of the detail from Government that we hope will show concrete support for the health workers, but it’s pretty clear at this point that the urgent need at the frontline has gone unacknowledged.”
Meanwhile the MHNS Committee has noted with concern recent comments by Health New Zealand Interim Chief Executive Margie Apa (from 44:37 in this video) and what they might mean for nursing in the new health system: “We can have another look at the way our teams work and how jobs are done”, she said. “There are tasks that can shift from medical practitioners to nursing, nursing to allied health.” After citing the growth of non-clinical vaccinators as part of the Covid response, Margie Apa continued, “In some areas we’ve got lots of nurses delivering a service that in other areas are delivered by technicians. That can be an awkward conversation for our workforces, but we’ve kind of got to go there.”
Our future is also shaped, however, by longer term trends. The MHNS Committee is pleased to publish in this newsletter reflections on the history of Mental Health Nursing from recently-retired Kaitiaki co-editor Teresa O’Connor. Her reflections below, originally composed for the (Covid-disrupted) 2021 MHNS Forum in Dunedin and titled “Can mental health nursing survive the zombie apocalypse?”, take the place of this month’s feature article.
Ultimately though, as American academic Peter Drucker quipped, the best way to predict the future is to create it. This issue of the MHNS Newsletter also reports on the “Future 2030” project, a collaboration between MHNS, Te Ao Māramatanga and the Directors of Mental Health Nurses national group to set the direction for mental health, addiction, and disability nursing. We hope you find something of interest in the following pages.
Introducing new Committee member Katie Neal
The MHNS Committee is delighted to welcome our newest member. Katie Neal, who joined us this month, qualified as a Mental Health Nurse in the UK in 2006. She has worked in acute and psychiatric inpatient intensive care, acute forensic inpatient, mixed rehab forensic inpatient and adult community mental health teams. She currently works as a Prison Liaison Nurse at Southern DHB.
Katie says, “Whilst I do not have any committee experience, I am a passionate Mental Health Nurse and am enthusiastic about the ongoing development of Mental Health Nursing in Aotearoa.”
Katie has been co-opted onto the Committee for the period up until the next MHNS Biennial General Meeting. The Committee, which comprises in addition Helen Garrick (Chairperson), Jennie Rae (Treasurer), Brent Doncliff (Secretary) and Grant Brookes (newsletter editor), is still looking for three more members. We invite any new, emerging leaders to join us. To express your interest, please click here for a nomination form.
Committee news
The MHNS Committee has met twice since our last newsletter in March. At our 17 March meeting, we reluctantly farewelled Margaret Daniela. In the context of increasing staff shortages, Margaret informed us that the demands of her role had grown to the point that she could no longer continue on the Committee.
Margaret was elected to the Committee in 2017. Among her many valuable contributions, she represented MHNS to the Chair of the 2018 Government Inquiry into Mental Health and Addiction, Ron Paterson, and filled the role of Committee Secretary. We thank Margaret for her service.
Committee members reported back about work on external bodies on behalf of MHNS. Brent Doncliff represented colleges and sections on the NZNO Membership Committee up until recently, and currently sits on the Mental Health and Addictions Employee Retention work group, created last year under the terms of settlement for the PSA Mental and Public Health Nursing MECAs.
Jennie Rae belongs to the NZNO DHB MECA Implementation sub-committee and the Constitutional Review Advisory Group (CRAG). CRAG signed off the member survey on the Constitution, which was sent to all NZNO members in April. MHNS is also represented on the NZNO project Address Violence and Aggression Against Nurses (AVAN), which is re-starting after an hiatus during the Covid pandemic.
Helen Garrick has been an advisor on the “Are You Ready?” advertising campaign, recently launched by the Ministry of Health to promote Mental Health and Addictions Nursing as a career. Helen also represents MHNS on “Future 2030” (see below for more about this project).
Lastly we revisited the idea of an online option to make it easier for NZNO members to join MHNS. This has now been actioned. We hope that current MHNS members will now encourage their colleagues to join.
A second, shorter meeting on 16 May focused mainly on planning for the next MHNS Biennial General Meeting, on a date to be confirmed, and on succession planning for the Committee – including the welcome news of Katie Neal’s co-option.
‘Future 2030’: A Framework for MH Nursing
It’s been 16 years since the publication of landmark report, the 2006 National Framework for Mental Health Nursing. Much has changed since that time. In recognition of this, a collaborative comprising NZNO MHNS, Te Ao Māramatanga and the Directors of Mental Health Nurses national group last year commissioned a project, Taking Mental Health, Addiction and Disability Nursing Forward to 2030. The aim of this “Future 2030” project was to prepare Mental Health, Addiction and Disability (MHAD) Nurses to make significant contributions to service delivery, their profession and in the lives of the people we serve and their whānau, over the next ten years.
The project contractors are now reaching the stage in the project scope where they are required to consult with MHAD nurses, followed by a presentation of draft recommendations.
As the project scope document states, “Within the scope of MHAD nursing, we demonstrate specialist skills across the variety of settings from acute, inpatient, community, and primary care to highly specialist settings such as maternal mental health and working with people with complex, traumatic life experiences. Combined with our professions ‘24/7’ approach to the nursing care of whaiora, we can lead in the specialist therapeutic skills that will be essential for the preparation of the future workforce and the challenges within the health environment.”
Twelve separate discussion papers are due to be released this month, on topics such as supervision, leadership and wellbeing. Consultation periods for these documents will be condensed, requiring a quick turnaround for any feedback. The MHNS Committee will distribute these discussion papers to MHNS members as soon as they are available.
IJMHN, Vol. 31 No. 3, June 2022
The MHNS Newsletter showcases the International Journal of Mental Health Nursing. Full access to the journal is a benefit of MHNS membership. To obtain an article, please email library@nzno.org.nz with the citation of the full text article you would like.
Issue Information
Issue Information
Pages: 445-446 First Published: 11 May 2022
Editorial
Supporting the emergent nursing workforce in the wake of the COVID-19 pandemic
Debra Jackson AO RN PhD FRCSI SFHEA FCNA, Kim Usher AM, RN, PhD, FACMHN
Pages: 447-449 First Published: 04 May 2022
Review Articles
Prevalence, associated factors and adverse outcomes of workplace violence towards nurses in psychiatric settings: A systematic review
Sun Joo Jang PhD, RN, Youn-Jung Son PhD, RN, CCAPN, Haeyoung Lee PhD, RN
Pages: 450-468 First Published: 13 November 2021
The effect of long-acting injectable antipsychotic medications compared with oral antipsychotic medications among people with schizophrenia: A systematic review and meta-analysis
Chizimuzo T.C. Okoli PhD MPH MSN APRN PMHNP-BC, Amani Kappi MSN RN, Tianyi Wang MS, Andrew Makowski DNP APRN PMHNP-BC, Andrew T. Cooley MD
Pages: 469-535 First Published: 20 December 2021
Original Articles
Exploring mental health clinicians’ perceptions of the Zero Suicide Prevention Initiative
Joanne E. Porter PhD, MN Grad Dip CC, Grad Cert Ed, Grad Dip HSM, BN, RN, Elissa Dabkowski PhD candidate, BN (Hons), RN, BPhysio, Owen Connolly MN, NP, GradDipBus, DipAOD, BN, RN, Valerie Prokopiv BA, Research Fellow
Pages: 536-543 First Published: 29 December 2021
Wait times in an Australian emergency department: A comparison of mental health and non-mental health patients in a regional emergency department
Sharene E. Pascoe BSocSc, MSc, Christina Aggar RN, BN(Hons), Grad Cert HE, PhD, Olivia Penman BPsychSci (Hons)
Pages: 544-552 First Published: 14 January 2022
A realist evaluation of weighted modalities as an alternative to pro re nata medication for mental health inpatients
Suzanne Dawson BAppSc (OT), PhD, Candice Oster BA (Hons), PhD, Justin Scanlan BOccThy, PhD, Jocelyn Kernot BAppSc (OT), PhD, Barry Ayling DipNg, GradDipMHNg, Katarzyna Pelichowski MBBS, Amelia Beamish BAppSc (OT)
Pages: 553-566 First Published: 07 January 2022
Contemporary perceptions and meanings of ‘the medical model’ amongst NHS mental health inpatient clinicians
Georgina L. Barnes BSc, MSc, DClinPsy, Maryam Z. Haghiran BSc, MSc, Derek K. Tracy MB BCh BAO, MSc, FRCPsych
Pages: 567-575 First Published: 07 January 2022
Sexual dysfunction in people treated with long-acting injectable antipsychotics in monotherapy or polypharmacy: a naturalistic study
Gema Martínez-Giner MD, Elisa Giménez-De Llano MD, Dolores Romero-Rubio RN, María José Abad-Pérez MHN, RN, Vanessa Sánchez-Martínez PhD, MHN, RN
Pages: 576-590 First Published: 01 January 2022
Experiences and challenges faced by community mental health workers when providing care to people with mental health conditions: A qualitative descriptive study
Yong-Shian Goh RN, RMN, MN, PhD, Qing Yun Jenna Ow Yong BSc (Hons), Shuenn-Chiang Soo MBBS, MMed (Psych), Po Ching Jennie Wan MSc, MSSc, Vincent Chee Keong Ng MSocSci, PhD
Pages: 591-600 First Published: 24 January 2022
Older residents’ perceptions of loneliness in long-term care facilities: A qualitative study
Pi-Hua Huang RN, MSN, Shou-Yu Wang RN, PhD, Sophia H. Hu RN, PhD, Yeu-Hui Chuang RN, PhD
Pages: 601-610 First Published: 03 February 2022
Rules and ward climate in acute psychiatric setting: Comparison of staff and patient perceptions
Marta Corbetta RN, BSC Nursing, Barbara Corso PhD, Carlo Alberto Camuccio RN, Msc, Msc Nursing
Pages: 611-624 First Published: 06 February 2022
An exploration of New Zealand mental health nurses’ personal physical activities
Glen Philbrick Master of Nursing (MN), New Zealand Diploma in Business, Nicolette Fay Sheridan PhD, Master of Public Health, Diploma in Occupational Health Practice, Kay McCauley PhD
Pages: 625-638 First Published: 14 February 2022
Prevalence and influencing factors of posttraumatic growth among nurses suffering from workplace violence: A cross-sectional study
Li Zeng BS, RN, Master Student, Xiangeng Zhang PhD, MD, Fang Wang RN, Jie Yun RN, Li Lai PhD, Man Jin BS, RN, Master Student, Guiling Liu BS, RN, Master Student, Yinong Qiu BS, RN, Master Student, Jialin Wang MSN, RN
Pages: 639-649 First Published: 12 March 2022
Measuring mental health recovery: Cross-cultural adaptation of the 15-item Questionnaire about the Process of Recovery in Spain (QPR-15-SP)
Jessica Marian Goodman-Casanova Master’s, Daniel Cuesta-Lozano PhD, Marta Garcia-Gallardo Master´s, Francisco Javier Duran-Jimenez, Fermin Mayoral-Cleries PhD, Jose Guzman-Parra PhD
Pages: 650-664 First Published: 11 March 2022
Mental health nurses’ experience of challenging workplace situations: A qualitative descriptive study
Kylie Cranage RN, MMentalHealth(Nurs), Kim Foster RN, PhD
Pages: 665-676 First Published: 28 March 2022
An evaluation of professional development for staff working with nursing students in distress
Colleen Ryan, Jennifer Mulvogue
Pages: 677-686 First Published: 04 March 2022
Protocol for a mixed methods process evaluation of the Promoting Resilience in Nurses (PRiN) trial
Minh Viet Bui RN, Elizabeth McInnes BA(Hons), Grad Dip App Sci, MPH, PhD, Gary Ennis RN, PhD, Kim Foster RN, PhD
Pages: 687-696 First Published: 13 March 2022
Mental health nurses perceptions of missed nursing care in acute inpatient units: A multi-method approach
Bindu Joseph PhD, RN, MSN, PG, Higher Ed, PBNN, Virginia Plummer PhD, RN, RM, FACN, FCHSM, CHE, Wendy Cross PhD, M Ed, B App Sc, RN
Pages: 697-707 First Published: 16 March 2022
How we say what we do and why it is important: An idiosyncratic analysis of mental health nursing identity on social media
Stephen McKenna Lawson RMN, MA, PgDip, BA
Pages: 708-721 First Published: 18 March 2022
Shared trauma during the COVID-19 pandemic: Psychological effects on Israeli mental health nurses
The revolt over broken promises to back-date Pay Equity for DHB nurses to 31 December 2019 is showing, once again, that union members are powerful when we organise and speak up.
For many DHB nurses, the broken back pay promises briefly brought back bad memories of 2018, when our MECA negotiators told us to accept substandard offers, refused to let us vote unless we sat through hour-long meetings, cancelled a strike that we had voted for and then, when we did strike, they let DHBs make a mockery of the Life Preserving Services agreements.
On 11 April, three days after releasing the proposed Pay Equity settlement, NZNO backtracked and announced a full legal review of the settlement agreement and the process leading up to it. The review validated what members had been saying. This was fantastic. It really was!
But why does it have to be so hard to get NZNO to act on our behalf, when We Are The Union?
We Are the Union. The Union is US.
This kind of thing mustn’t happen again. We need to rewrite the rules, so that NZNO is driven by its members. And between now and 30 April, with the Constitutional Review, we have a golden opportunity to do just that.
What is the Constitution, and why does it matter?
Weighing in at a hefty 49 pages and written in dense legalese, the NZNO Constitution is a document that most people have never read. Who can blame them?
And yet the Constitution is a matter of importance for every fee-paying member of NZNO. This is because it:
Defines the purpose and objectives of NZNO (what it’s for, and what it will do)
Sets out the rights of union members (along with our responsibilities)
Determines who has the power to do what, inside NZNO
Since NZNO is an incorporated society and a union, its Constitution is a legally binding document. Any member is actually able to go to court or to the Employment Relations Authority if they believe the Constitution has been breached. And now this document is up for review.
All NZNO members were emailed a link on 1 April to a Member Survey about the Constitution, open until 30 April. The survey is 40 pages long! I know, because I printed it to PDF using A4 paper size. Who’s got time for a 40-page survey?
The good news, as explained at on page one, is that, “You do not need to answer all questions in order to provide valuable feedback. There may be specific issues of concern to you that you would like to focus on.”
So if you read no further in this article, please at least click on that link in your email and go to Section 4 of the survey, to speak up for the “Objects of the NZNO” that you want to see prioritised.
Along with the Board election later this year (more on that below), the survey is our biggest chance to exercise our rights as as members and speak up for a membership-driven union. If you’d like to see how I answered all the survey questions, click here. If you want to understand my perspective on problems in the Constitution and the rule changes needed to empower members, please read on. I am proposing ideas which you might like to put in your survey responses, in the following areas:
When Board members Anne Daniels, Katrina Hopkinson and Sela Ikavuka resigned in April 2020, just eight months after being elected, many NZNO members were shocked to learn that they were bound by a “gagging order”. “Right from the start”, the trio wrote, “we were required to sign a confidentiality agreement before our first meeting.”
That’s right – the elected leaders NZNO are barred, under threat of legal action, from sharing information with the membership who vote them into office. It hasn’t always been this way. Up until a decade ago, all NZNO Board members used to produce regular reports for the members they represented.
But NZNO today has a problem with openness and honesty, and the problem starts at the top. Last year, the Board refused to release an external review of its performance. Hundreds of members signed a petition calling for its release. “As a transparent, member-led organisation”, said petition organiser and NZNO delegate Al Dietschin, “we believe every member who wants to see this review, which was paid for by NZNO members’ fees, should be able to access it on the website.” The Board dismissed their call.
Agendas and minutes of Board meetings are supposed to be made available to the membership and staff, after a binding motion was passed in 2016 by NZNO delegates unhappy at the Board’s lack of accountability and transparency. But last year, the Board simply ignored that vote and went back to operating in secrecy. Their secrecy has included a serious lack of detail about how all our member fees are spent.
Perhaps the most significant report for NZNO in recent years, the Independent Review of the 2017/18 DHB MECA campaign which led to major changes in NZNO’s approach to bargaining, was also initially withheld. NZNO chief executive Memo Musa said the report would “remain confidential and not be shared with others without the express permission of the chief executive and industrial services manager.” It was only published, in a redacted form, thanks to the organising efforts of hundreds of members who forced its release.
This culture of secrecy filters down from the top and affects other parts of NZNO, in ways big and small. The secretaries and chairs of NZNO Colleges and Sections, for instance, aren’t even allowed to know the names of the people on their own membership list. Delegates in the same workplace are prevented from talking with each other (and they members they represent) because they can’t get names or contact details.
The withholding of information is a way of actively disempowering NZNO members. In place of open and honest communication, we have even been fed self-serving misinformation. In 2019, a very strange email to all member groups from the Board said, “The Board wishes to clearly state that it is united. Contrary to some suggestions that have been made, the Board is neither dysfunctional nor divided.” Meanwhile the external review, which later leaked despite the Board’s attempts to suppress it, said that during this time the Board was in “a governance crisis”, crippled by internal conflicts and unethical conduct, to the point where it couldn’t say what value (if any) it was adding to the organisation.
“I want to see improved transparency”, said NZNO Vice President Nano Tunnicliff in her election profile statement last year. The Constitutional Review provides an opportunity to achieve this. The Constitution should set out clearly the rights of NZNO members to information about our own union. NZNO’s culture of secrecy is out of step with other similar organisations, current understanding about good governance and recent law changes.
This month, the Incorporated Societies Act 2022 came into force. This Act updates the legislation governing entities like NZNO, and expresses the expectations of New Zealanders around open and transparent governance. Section 80 of the Act sets out for the first time a legal right to information held by incorporated societies (including unions) for members of that society. If the officers of a union refuse an information request, members can now get a court order for its release. There are only a few limited grounds for refusing a request to release information to a member. One of them is if it says that information can be withheld in an organisation’s constitution.
After learning from the Independent Review of the 2017/18 DHB MECA campaign, last year’s MECA bargaining was refreshingly different. DHB Sector members were given frequent updates, containing all the information they needed to make informed decisions for themselves. Information previously marked “confidential”, such as the detailed results of member votes, was now made available. NZNO negotiators were accessible for the first time on social media, and answered questions.
It’s time to make this the norm, for all of NZNO. We can do that by speaking up for rules to empower NZNO members in section 7 of the survey. I suggest that the Constitution should explicitly state, under “Rights and Responsibilities of Membership”, that union members have a right to information held by NZNO, subject only to the grounds for refusing information requests provided in the Incorporated Societies Act 2022.
Genuine democracy
NZNO today is stuck, part way through a transformation into a genuinely democratic organisation. The Constitution currently says that all members have the right to vote on some matters, but decision-making on other matters remains secretive and undemocratic. Section 6 of the Member Survey is our chance to speak up for changes to strengthen our union democracy and member voice.
Enabling all members to vote is a relatively recent development for NZNO. It was not until 2018 that the system of “One Member, One Vote” was introduced, finally empowering every member to vote online for NZNO policy and rule changes. That same year, online voting was introduced in MECA bargaining. When online voting was first raised, it met with strong opposition from NZNO leaders. Now we have to wonder what all the fuss was about. It seems strange to think that prior to 2018, the only members allowed to vote on these things were those able to attend long meetings, in person.
But for other decisions which affect NZNO members, voting by people able to attend long meetings is still in place. This is the case for Annual General Meetings and for two Special General Meetings of the union held in 2019. Whether I like it or not, this part Constitutional Review is bound up with my own story as NZNO President, as these SGMs were both about me. But as someone who has campaigned long and hard against undemocratic features of the Constitution for over a decade – in print, on line and at meetings, even drafting a remit for a constitutional review (later superseded) in December 2019 – my ideas now are not simply a reaction to my own recent experiences.
The problems with the current system of voting at meetings “on a representational basis” are that:
Under Section 30 of the Constitution, just 33 people (out of the 55,000 members in NZNO) are allowed to vote. They are the representatives of the 11 Regional Councils, 20 Colleges and Sections, the National Student Unit and Te Rūnanga
These 33 representatives (generally the Chairpersons) get the number of votes equal to the number of members in the group they’re representing. This means you can have one rep casting the vote for up to 15,000 members
The largest five membership groups comprise over half of the membership, meaning just five representatives could make a “majority” decision for all of NZNO
Yet, there is no requirement for the “representatives” to consult the membership they’re voting on behalf of – and many have been quite open about the fact they don’t consult – or to vote in accordance with the wishes of their members, if these are known
There’s no way for members to know how their representatives even voted, because it’s “secret”
And the kicker? The eleven Regional Council Chairs, who wield two thirds of the total vote at AGMs and SGMs, aren’t even elected by the membership of their Region
Members can see that an unelected handful casting thousands of secret votes is an open invitation to corruption, and this has contributed to a breakdown of trust in NZNO. It’s also a pretty rotten system that so few can make a decision that’s paraded around as a democratic decision of the membership.
If this wasn’t reason enough, the system of voting “on a representational basis” is now broken completely in a time when meetings are being held virtually by Zoom. The NZNO Annual Report 2020/21 and the audited financial statements, for instance, were accepted through an AGM ballot where only a minority of the eligible reps voted on behalf of their members at all.
Given this, I have two strong suggestions for responses in Section 6 of the survey. Firstly, people should clearly state that we must keep the “One Member, One Vote” system. Because believe it or not, there is a push at the top of NZNO to remove this from the Constitution and go back to making decisions about remits on a “representational basis” at meetings. Those driving the move backwards say that democracy is inherently “racist”, against Māori.
Their argument rests on the assumption that all Māori think and vote the same way, and that Pākehā and other tauiwi always vote against them. Because Māori are a minority, the argument goes, they will always be outvoted and always lose out.
This argument, however, stereotypes Māori and is not supported by the evidence. Voting for NZNO Board members, for instance, is an area where the “One Member, One Vote” system has applied since 2011. At the last election in 2019, democracy produced wins for Māori candidates. The following year, in an all-member ballot using the “One Member, One Vote” system, a remit giving Māori NZNO members the power to veto anything in future which affects Te Rūnanga or is inconsistent with their rules (Ngā Ture) attracted overwhelming democratic support. This remit to empower Māori NZNO members, which I wrote before stepping down as NZNO President, passed with 73 percent of the vote.
It can sometimes happen that democratic, majority rule systems fail to adequately respect minority rights. This is why protections underpinned by Te Tiriti o Waitangi – like giving Māori members veto power over things which affect them – are needed.
But democracy is not inherently racist. Dressing up opposition to democracy in the garb of anti-racism is just disingenuous. As the world looks on in horror at attempts to suppress democracy in Ukraine, we need to be very clear that democracy is the best system of governance we have. Since the introduction of online democratic voting in 2018, it has strengthened our union, massively increased participation, delivered better outcomes and improved member satisfaction. It is certainly superior to the secretive, unaccountable decision-making that goes on at meetings.
So in addition to stating clearly in Section 6 of the survey that we must keep the current “One Member, One Vote” system, members should also tick “yes” to support “One Member, One Vote” on AGM matters and also tick the box to say that “Voting at a special general meeting should be… By one member, one vote to be carried out electronically or by post.”
Kaitiakitanga & servant leadership
The dissatisfaction over the Board’s lack of transparency and the damning assessment of its ethics in the recent external review has fuelled a widespread suspicion that in recent years, the NZNO Board has been driven by personal agendas – not by the needs of the membership. In my experience, this suspicion is well founded. Spending a quarter of a million dollars of members’ money on the Board’s own legal battles in 2018-19 must rank as a scandal, all on its own. We need a board who hold fast instead to values like kaitiakitanga, acting as custodians serving on behalf the membership for a time, rather than as owners of the organisation who would use its resources for their own ends.
The culture and values of a Board, whether that’s a culture of service or an inflated sense of superiority and entitlement, is shaped by many factors. But in the case of the NZNO Board, they include aspects of the Constitution.
Section 5 of the Member Survey focuses on the Board. The second question in this section begins, “The current term for board members, with the exception of the Kaiwhakahaere and the Tumu whakarae is three years, with a right of re-election for a further consecutive three years in any one position. A director may serve up to two terms in any one position. The maximum consecutive terms on the board in any combination of positions is four. Following two terms in any one position or four terms in a combination of positions, a director may be eligible to stand for office again after a break of two years.”
So as the survey explains, the Constitution currently limits how long the President, Vice-President and the non-officer directors can remain in their positions.
What the survey does not mention is the very next clause in the Constitution: “… The term of the Kaiwhakahaere and Tumu whakarae Directors shall be three years, with a right of re-election for a further consecutive three years, and may be eligible to stand for office again every three years thereafter.” In other words, there are no limits on how long the Kaiwhakahaere and Tumu Whakarae can hold hold office. Nor does the survey mention the six figure salaries paid to the elected officers.
And the survey does not mention how the Kaiwhakahaere and Tumu Whakarae are elected, either. As stated in Schedule Three of the Constitution, these positions are elected at the Hui ā-Tau – which is run each year under the rules of Te Rūnanga (Ngā Ture). In accordance with the principle of tino rangatiratanga, Ngā Ture are determined by solely by Māori members of NZNO. They are not up for wider input as part of the Constitutional Review. However, Ngā Ture are referenced in the NZNO Constitution and need to be read alongside it, as these rules of Te Rūnanga provide relevant additional context.
Ngā Ture state that to be eligible to stand in elections for the position of Kaiwhakahaere or Tumu Whakarae, candidates must have held a position at Te Poari within two years of applying. In other words, while a call for nominations for these positions goes out every three years to all 4,000 members of Te Rūnanga, the only people eligible to stand (apart from the two incumbents) are two nursing students from Te Rūnanga Tauira, or (realistically) the eleven regional representatives who make up the rest of Te Poari.
This tiny pool of potential candidates (numbering just eleven, or perhaps a couple more given turnover in these positions in a two year period) are all people who have served loyally under the incumbent office-holders – who also happen to control the budget for travel and accommodation for the delegates to Hui ā-Tau, and control who may speak at Hui-ā-Tau, where the couple of hundred voters who’ve been funded to attend elect the Kaiwhakahaere and Tumu Whakarae.
These rules go some way to explaining why, in the last 13 years, the position of Kaiwhakahaere has never been the subject of a contested democratic election – and probably won’t be in the future, either.
The term limits which specified how long the Kaiwhakahaere and Tumu Whakarae can hold hold office were removed from the Constitution in 2017. The rationale for this was something I went along with at the time, and I lent my support to the change. But with the benefit of hindsight, the key argument – that the pool of Māori RN members with the level of skill and knowledge required is so small, that two individuals must be allowed to hold office indefinitely – does a gross disservice to the amazing strength and leadership abilities of Māori nurses as a whole.
In combination with the strict limitations on eligibility for office in Ngā Ture and the introduction of six figure salaries for NZNO officers, the consequence of this Constitutional change – perhaps unintended – has been to effectively turn what should be kaitiaki roles into careers and “jobs for life”. This is having a negative impact on the development and emergence of new Māori nursing leaders, and creating psychological and cultural shifts on the Board which divert its focus away from serving the membership.
Servant leadership is a leadership philosophy in which the goal of the leader is to serve. A servant leader shares power, puts the needs of members and staff first and helps people develop and perform as highly as possible. Instead of the people working to serve the leader, the leader exists to serve the people. This culture is what we need to restore to the NZNO Board, and Constitutional change can be a part of that.
The last question in Section 5 of the Member Survey asks, “If I could propose one process involving the Board that would benefit me as a member, that process would be…”. I suggest that an answer could be, “To apply equal term limits for all Board members so they each understand their stewardship role, as custodians serving on behalf the membership for a limited time only.”
Engagement and Belonging
Section 3 of the Member Survey will strike virtually all NZNO members as odd. Under a heading of “Connection to the NZNO”, it begins by asking whether you belong to a Regional Council. Faced with this question, most NZNO members will wonder, “What’s a Regional Council?”.
In this way, the survey unintentionally highlights what is a fundamental disconnect between NZNO members and the structures of our union. This disconnect is based on flaws in the Constitution. We now have the opportunity to fix these flaws and build other member structures which support engagement and belonging.
The eleven NZNO Regional Councils were created in 1989. They replaced the 54 “branches” in the old New Zealand Nurses Association (NZNA), shortly before it transformed into the NZNO we have today. Under the NZNO Constitution, Regional Councils have a lot of power. Not only do the Council Chairs wield thousands of votes each in NZNO meetings (see above), they also control the submission of remits for the “One Member, One Vote” process and approve candidates wishing to stand for the NZNO Board.
The flaws in the system have been well understood for many years. Back in 1998, the NZNO Conference requested that the effectiveness of Regional Councils be reviewed. The review concluded that Regional Councils were not effective, but the resulting changes were minor.
In 2003, delegates to the NZNO AGM went further. They debated a paper proposing significant change to the structure of NZNO. The discussion paper said:
“Regional Councils have not been effective in representing members and have been reviewed in the past.
At present there are 11 Regional Councils. The Committee reviewed the attendance over the past 12 months of six of those Regional Councils; Central, Bay of Plenty, Auckland, Midlands, Wellington and Southern. All met two- monthly. The lowest attendance was three persons, the maximum attendance was 23 (Southern). No other Regional Council meeting had an attendance of 20 or more persons. The average attendance of the Regional Councils over the 12 month period ranged between under 10 to a little over 14 (Auckland). These are extremely low numbers and cannot give any confidence that decision making structures based around Regional Council are inclusive, democratic and participatory.”
The problem has only gotten worse since 2003. In 2010 the official centennial history of NZNO, Freed to Care, Proud to Nurse, described the replacement of union branches by Regional Councils:
“This restructuring was seen by NZNA leadership as better representing the majority of members, who now worked across multiple workplaces. It was perceived by the membership, however, as the destruction of the organic channels that they had created. In fact, the imposed structure was never to function in the comfortable, rhythmic way that the old branches had.”
Today, although NZNO membership has grown to the point that the Regional Councils are supposed to represent thousands or even tens of thousands of members each, most still struggle to get meeting participation numbering in double digits.
I need to stress that the fault in this system does not lie with the member volunteers who keep the Regional Councils running. Regional Council members are among the most dedicated NZNO members, who work incredibly hard to try and make them work. The problem is, they’re working in a structure that’s never worked since it was first created, 33 years ago, and is now broken beyond repair.
“The main drivers behind our present structure were legislative requirements in the Labour Relations Act 1987 and the Employment Contracts Act 1991”, observed the 2003 NZNO AGM discussion paper. These laws were repealed decades ago. NZNO Regional Councils are relics of a bygone age. Divorced from the conditions which led to their creation, they no longer made sense in 2003, and they make even less sense now.
Other problems with NZNO structures flow on from this. The Membership Committee, which is first mentioned in Section 2 of the Member Survey, was created in 2012 “to advise the board”, due to member concerns that the Board would become remote and unaccountable.
It hasn’t worked. The Board did become remote and unaccountable. The Membership Committee was never to fulfil the key functions in its original Charter of:
“Providing further insight into the views and needs of the diverse membership of NZNO and provide a link to the local level
Ensuring the NZNO is responsive to the needs and issues of members
Receiving and considering the summary of Board meetings and providing feedback”
There are two reasons for this. Firstly, because the Board would simply refuse requests to meet, or to provide a summary of their meetings. But also because the Membership Committee is based largely upon the unrepresentative, disconnected Regional Councils.
Despite my best efforts during six years on the Membership Committee, in various roles, I watched it get captured by the agendas of the Board, succumb to the culture of secrecy at the top and finally adopt a new Charter in 2020 which deleted its original purpose. Today almost half the positions on the Membership Committee sit vacant, partly as a result of its irrelevance. Even with the added inducement of fully funded travel, meals and accommodation, paid leave and reimbursement of meeting expenses, the vacancies cannot be filled.
Under “General Understanding of Constitution”, Section 2 of the survey asks about “the most important functions of the Membership Committee”. I suggest that an answer could be: “Representing the views and needs of the diverse membership of NZNO and providing a link to the local level, and ensuring the NZNO is responsive to the needs and issues of members, which it cannot possibly do under current Constitutional arrangements.”
But outside of the Regional Councils and Membership Committee, there are functioning structures where NZNO members do engage and feel a sense of belonging, such as the Colleges and Sections. The functioning structures also include the Worksite Organising Committees (aka WOCs, or the “monthly delegates meeting”), led by an elected Convenor (aka “Lead Delegate”), and the National Delegates Committees (NDCs). The WOCs and NDCs provide crucial input into on NZNO’s industrial strategies at all levels and guide our negotiating teams. You may be surprised to learn that this democratic structure, where members are highly engaged doing vital NZNO work, is described in the NZNO Delegates Handbook but has no formal powers under the Constitution.
The Colleges and Sections are a place where members feel a sense of belonging and engage in the work of NZNO.
The delegates to the NZNO AGM back in 2003 decided to commission a full structural review. The 2004 Report of the Structural Review Committee proposed solutions which still make sense today. It said:
“The Issue
The Committee recognises that much of the activity and work of NZNO carried out by members occurs at workplaces, Colleges and Sections and it seems appropriate to locate decision making where membership activity occurs…”
“Proposed Changes
It is proposed that as far as possible NZNO should devolve its decision making and relate to, consult with, and organise its membership through Workplaces, Colleges and Sections.
The Committee proposes that Workplace Committees be formalised in the governance structure of NZNO. Under the proposed model general membership participation and decision making would be devolved to Workplaces, Colleges and Sections. The primary flow of communication would be directly from workplaces and Colleges and Sections to national structures and vice versa.
It is proposed that existing Regional Councils… be retained for a period of two years and then reviewed.”
Section 3 of the Member Survey asks, “The benefits that I obtain from a Regional Council are as follows”. Be honest. If the answer is nothing, say “nothing”. Then in Section 7 of the survey, which asks you to, “Indicate below if you have any comment in respect of a specific structure”. You might like to write something along these lines under “Regional Councils”:
“Back in 2004, at the time of the last NZNO structural review, Regional Councils selected the members of the NZNO Board and did all the voting on remits. Both of these democratic functions have now been transferred to the “One Member, One Vote” system. As mentioned in responses under Section 6 of this survey, voting at AGMs and SGMs also needs to be done according to “One Member, One Vote”. The Regional Councils did have a (relatively small) role in organising Regional Conventions, but these have now been cancelled.
The functions remaining – which largely consist of proposing remits, endorsing candidates wishing to stand for Board, assisting with implementation of NZNO policies and strategies, electing Membership Committee reps and working in partnership with Te Rūnanga – should be devolved to Colleges, Sections and constitutionally defined Worksite Organising Committees, in accordance with the recommendations of the 2004 Structural Review Committee. Regional Councils can then be wound up.”
What’s next?
This article has suggested a few ideas for members to include in their responses to the current Member Survey on the NZNO Constitution. But it’s far from an exhaustive list. For anyone interested, my complete Member Survey responses are available (for a cheeky copy/paste) here.
Section 8 of the Member Survey asks if there are, “any other comments you would like to make in respect of the Constitution of the Organisation.” You might like to comment that NZNO is the only professional association and registered union in Australasia (and possibly the world, apart from the Royal College of Nursing in the UK) which has a Chief Executive Officer. There appears to be no valid reason for this, although it does lead to a much higher salary for NZNO’s most senior manager, funded of course by our membership fees. In fact, it looks like a bit like a colonial hangover. The CEO role prescribed in Section 20 of the Constitution should be re-scoped, possibly as National Secretary, which was the title held by our current CEO as head of his previous registered union and professional association from 2008-2022.
Some of the things mentioned in the Member Survey – like the questions about Partnership under Te Tiriti o Waitangi in Section 6 – relate largely to personalities and practices, however, which won’t be fixed by changing the Constitution. And any Constitution is only as good as the people who operationalise it. The people who have been dominating the NZNO Board for years have trampled on our union’s system of rules and the values which underpin it – much like what President Donald Trump did with the US Constitution (even to the point of seeking to overturn a democratically-elected NZNO President).
So as well as participating in the current Member Survey before 30 April, and considering the suggestions for survey responses in this article, I hope that union members will also participate in the upcoming election for the NZNO Board. Come August, seven of the eleven Board seats will be up for grabs. For the reasons already stated, this year we need to elect people who support the ongoing transformation of NZNO. We need bicultural servant leaders committed to openness and honesty, genuine democracy and engagement and belonging for NZNO members.
















{kind=link}
{kind=link}